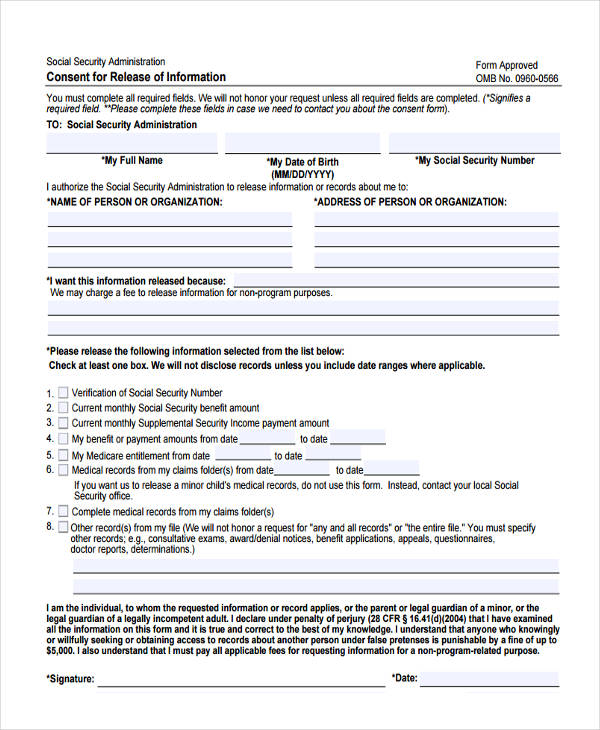
General Release Blank Authorization To Release Information Form - Meet your privacy obligations under hipaa with this authorization to release medical information form. This consent form will expire on (date)_____________ or __________ days from the. This form is to provide the military treatment. Always stay on top of your patient's. Sample authorization for release of confidential information. To request release of medical information please complete and sign this form i, ____________________________________hereby.
This form is to provide the military treatment. Always stay on top of your patient's. To request release of medical information please complete and sign this form i, ____________________________________hereby. Meet your privacy obligations under hipaa with this authorization to release medical information form. Sample authorization for release of confidential information. This consent form will expire on (date)_____________ or __________ days from the.
Sample authorization for release of confidential information. To request release of medical information please complete and sign this form i, ____________________________________hereby. Always stay on top of your patient's. This form is to provide the military treatment. Meet your privacy obligations under hipaa with this authorization to release medical information form. This consent form will expire on (date)_____________ or __________ days from the.
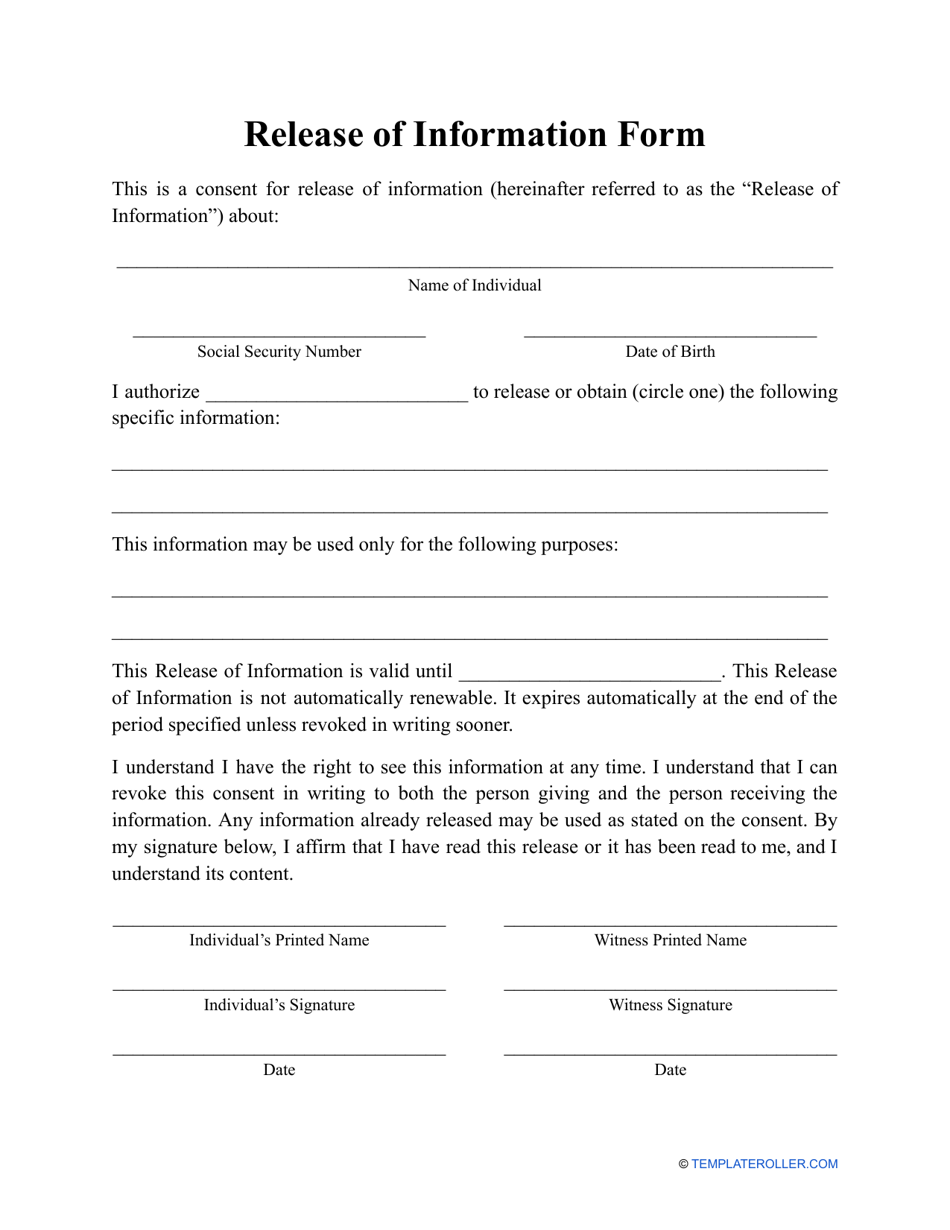
Release of Information Form Fill Out, Sign Online and Download PDF
This form is to provide the military treatment. This consent form will expire on (date)_____________ or __________ days from the. Sample authorization for release of confidential information. Meet your privacy obligations under hipaa with this authorization to release medical information form. Always stay on top of your patient's.
FREE 14+ Release Authorization Forms in PDF MS Word Excel
Sample authorization for release of confidential information. Meet your privacy obligations under hipaa with this authorization to release medical information form. Always stay on top of your patient's. To request release of medical information please complete and sign this form i, ____________________________________hereby. This consent form will expire on (date)_____________ or __________ days from the.
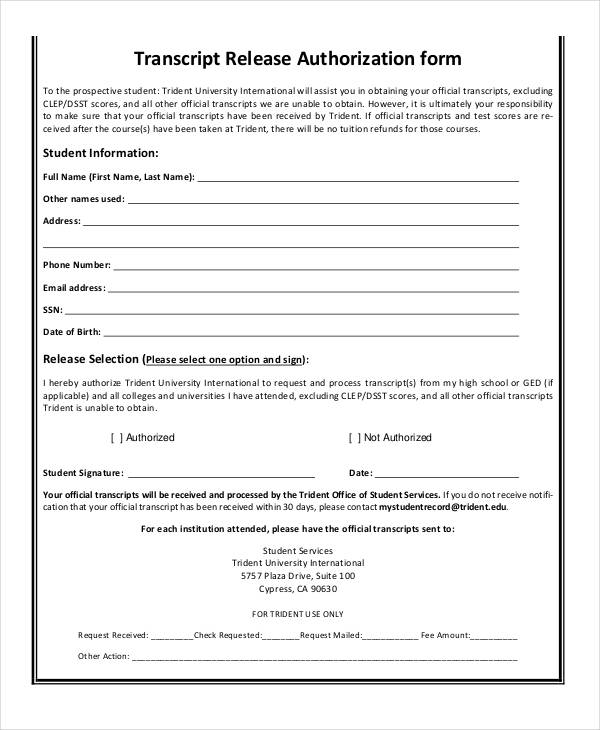
FREE 9+ Sample Release of Information Forms in MS Word PDF
Always stay on top of your patient's. This form is to provide the military treatment. This consent form will expire on (date)_____________ or __________ days from the. Meet your privacy obligations under hipaa with this authorization to release medical information form. To request release of medical information please complete and sign this form i, ____________________________________hereby.
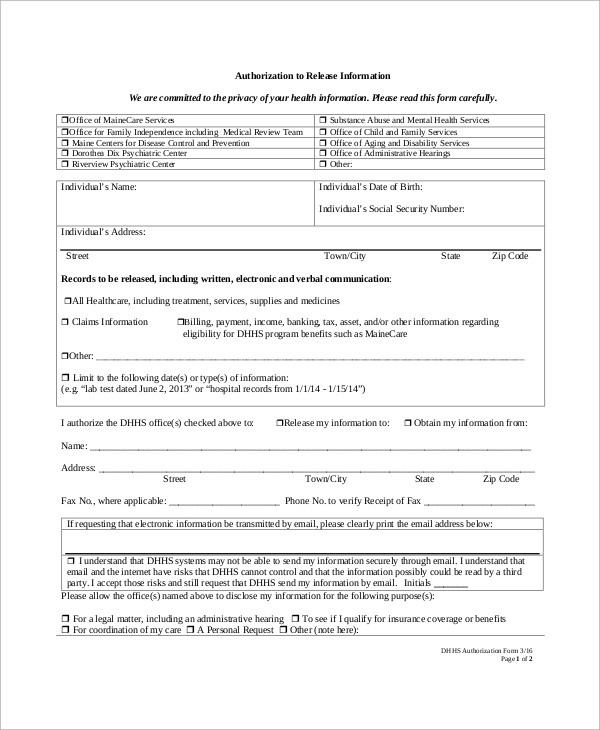
Printable Authorization To Release Information Form Printable Forms
To request release of medical information please complete and sign this form i, ____________________________________hereby. This form is to provide the military treatment. Sample authorization for release of confidential information. Meet your privacy obligations under hipaa with this authorization to release medical information form. This consent form will expire on (date)_____________ or __________ days from the.

Printable Blank Authorization To Release Information Form
To request release of medical information please complete and sign this form i, ____________________________________hereby. This consent form will expire on (date)_____________ or __________ days from the. Always stay on top of your patient's. This form is to provide the military treatment. Meet your privacy obligations under hipaa with this authorization to release medical information form.

Blank Release Of Information Form
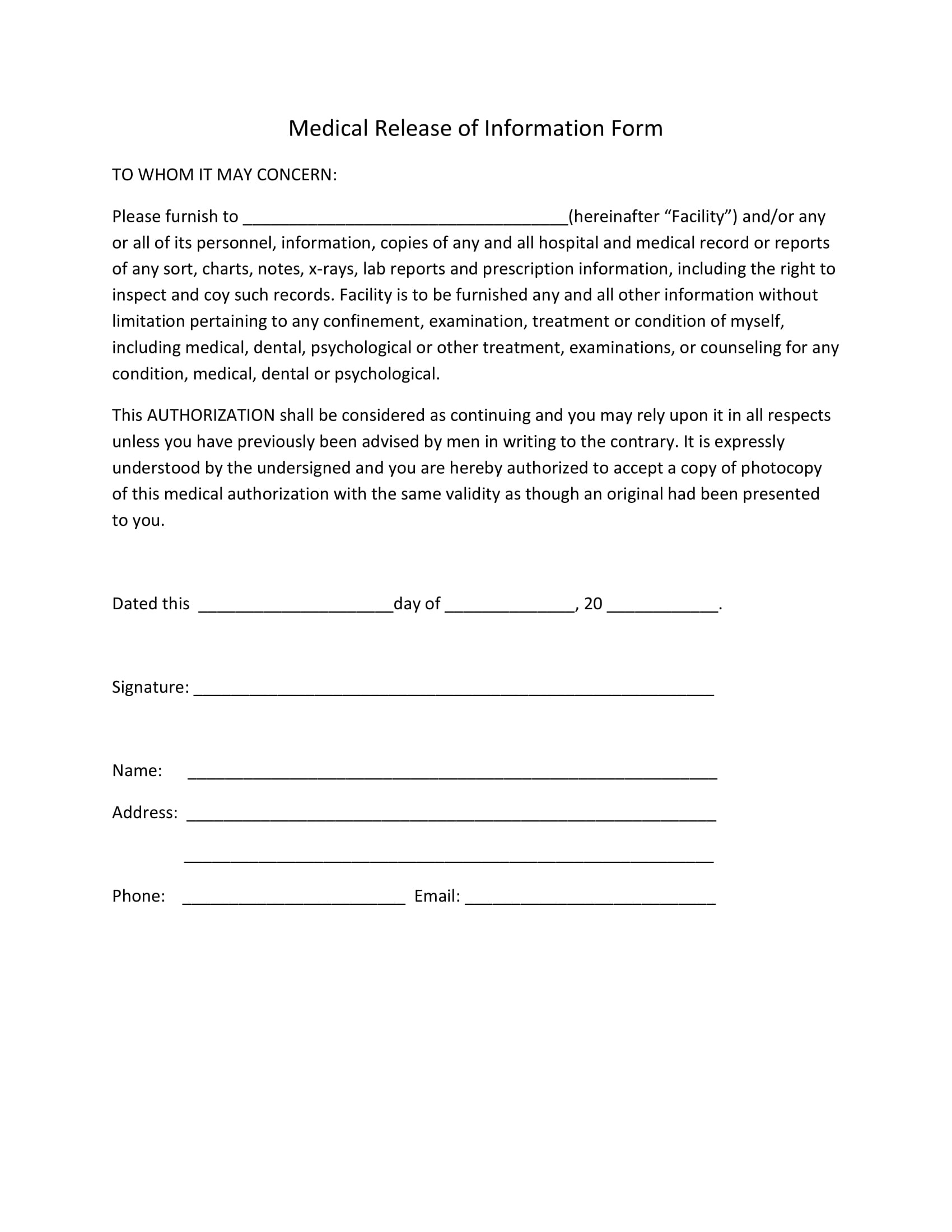
Meet your privacy obligations under hipaa with this authorization to release medical information form. Sample authorization for release of confidential information. To request release of medical information please complete and sign this form i, ____________________________________hereby. This consent form will expire on (date)_____________ or __________ days from the. This form is to provide the military treatment.
Printable Blank Authorization To Release Information Form
Sample authorization for release of confidential information. Meet your privacy obligations under hipaa with this authorization to release medical information form. To request release of medical information please complete and sign this form i, ____________________________________hereby. This consent form will expire on (date)_____________ or __________ days from the. This form is to provide the military treatment.
Blank Printable Authorization To Release Form Printable Forms Free Online
Meet your privacy obligations under hipaa with this authorization to release medical information form. Sample authorization for release of confidential information. To request release of medical information please complete and sign this form i, ____________________________________hereby. This consent form will expire on (date)_____________ or __________ days from the. This form is to provide the military treatment.
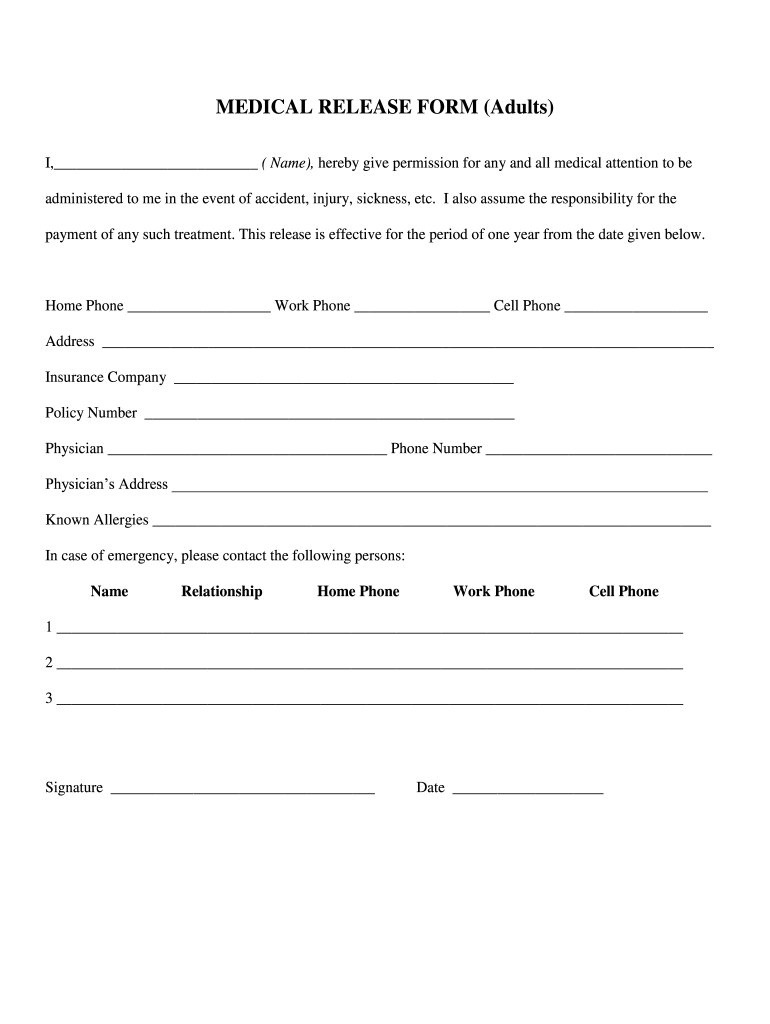
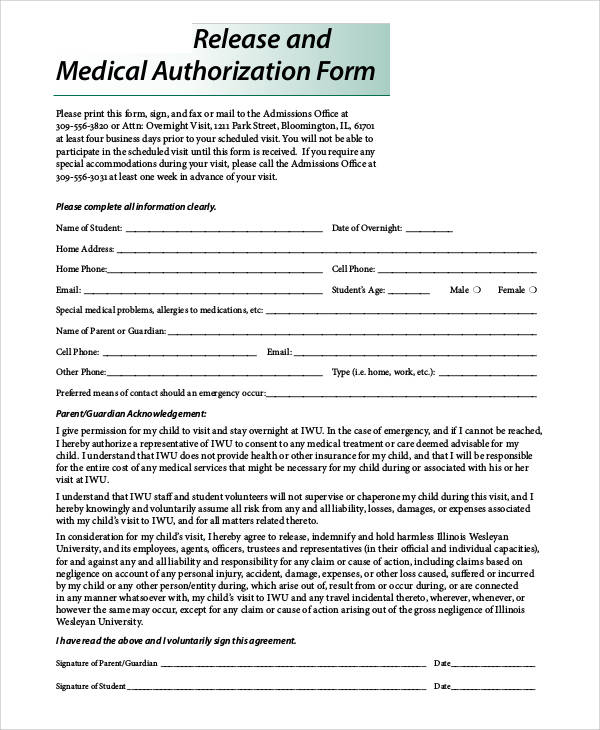
Medical Release Forms
This form is to provide the military treatment. Meet your privacy obligations under hipaa with this authorization to release medical information form. Sample authorization for release of confidential information. This consent form will expire on (date)_____________ or __________ days from the. Always stay on top of your patient's.
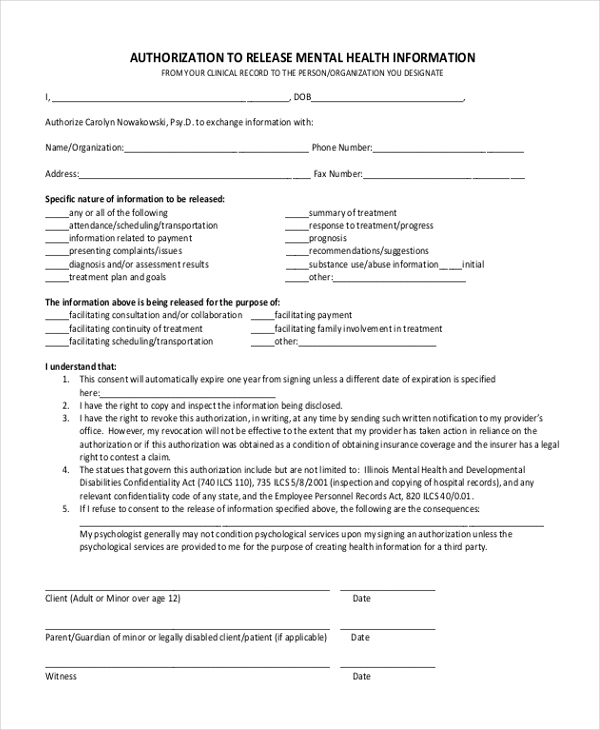
Free Mental Health Release Of Information Form
Sample authorization for release of confidential information. Meet your privacy obligations under hipaa with this authorization to release medical information form. Always stay on top of your patient's. To request release of medical information please complete and sign this form i, ____________________________________hereby. This consent form will expire on (date)_____________ or __________ days from the.
This Consent Form Will Expire On (Date)_____________ Or __________ Days From The.
Sample authorization for release of confidential information. To request release of medical information please complete and sign this form i, ____________________________________hereby. This form is to provide the military treatment. Always stay on top of your patient's.